
Major bleeding
- Hematoma and hemoperiteneum requiring transfusion occurs after 1% of paracentesis5
- Select a safe location for needle entry by avoiding
- Rectus abdominus muscles contain large epigastric arteries
- Surgical scars which often have neovascularization
- Engorged subcutaneous veins
- Abdominal wall bruises and hematomas
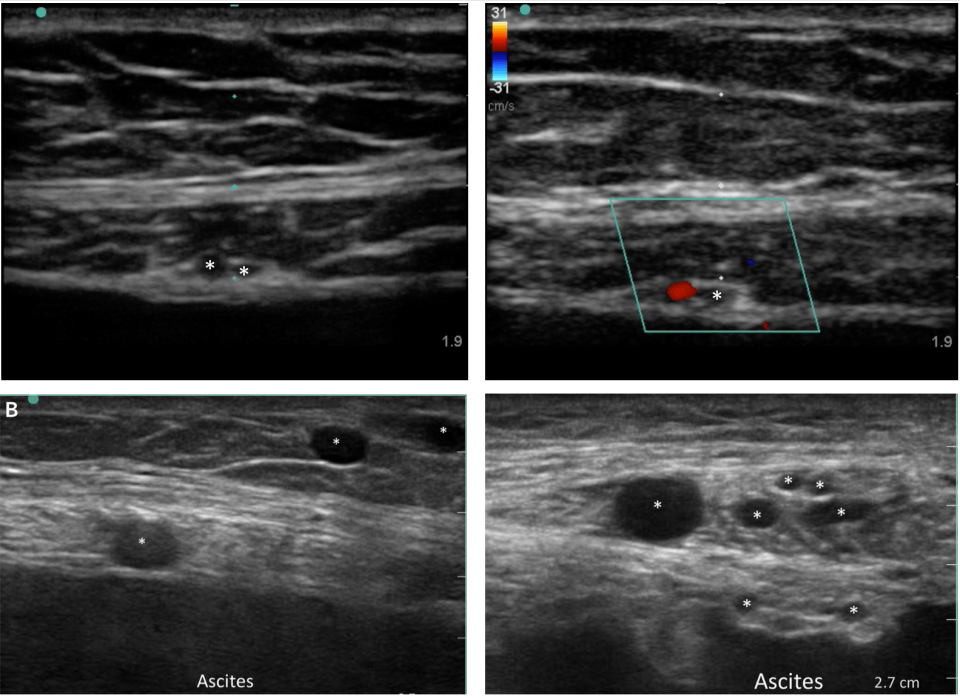
- Use the linear (vascular) probe to assess for subcutaneous vessels prior to needle puncture
- 1 institution found vessels in the path of their needle 10% of the time, and reduced major bleeding with routine use of the linear US probe7
- See previous page for transfusion indications
Acute kidney injury, hypotension and hyponatremia
- Large volume paracentesis should be avoided in AKI and hemodynamically unstable patients1
- Post paracentesis there is large fluid shift back into the peritoneum, reducing the effective arterial circulation
- Prevention with albumin
- A meta-analysis demonstrated that albumin significantly reduced post-paracentesis mortality from 14% -> 12%1
- If ≥ 5 liters are removed, 6 gram of albumin should be given for every liter removed 1-4
- 1 bottle of 25% albumin has 25gm in 100ml
- For example, if 8L are removed, give 48 grams of albumin which is about 200ml of 25% albumin
- Albumin should be given during the procedure or immediately after
- Consider albumin in all cirrhotics with baseline hypotension
Bowel perforation
- Occurs in less than 0.5%5
- Prevention
- Avoid surgical scars where adhesions may form
- Use ultrasound to find the deepest fluid pocket of at least 3cm
- Most perforations cause self-limited peritonitis that does not require surgical intervention
Persistent ascites fluid leakage
- Occurs in up to 5% of patients5
- Prevention
- Offsetting the skin puncture and the peritoneal puncture should decrease the risk of leakage, but it has never been studied 6
- 2 techniques4
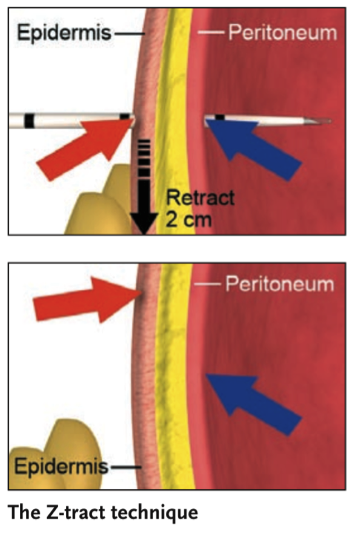
- Z track
- pull the skin 2cm with your non-dominate hand during needle entry
- Angled insertion technique
- Insert the needle at a 45°
- Be sure your fluid pocket seen on US can accommodate this needle trajectory
- Z track
- Treatment
- Control and monitor fluid output with an ostomy bag
- If persistent, and you can place a suture to close the skin
Next Page
References
- Bernardi, M., Caraceni, P., Navickis, R.J. & Wilkes, M.M. Albumin infusion in patients undergoing large-volume paracentesis: a meta-analysis of randomized trials. Hepatology 55, 1172-81 (2012).
- Gines, P., Cardenas, A., Arroyo, V. & Rodes, J. Management of cirrhosis and ascites. N Engl J Med 350, 1646-54 (2004).
- Runyon, B.A. Management of adult patients with ascites due to cirrhosis: an update. Hepatology 49, 2087-107 (2009).
- Thomsen, T.W., Shaffer, R.W., White, B. & Setnik, G.S. Videos in clinical medicine. Paracentesis. N Engl J Med 355, e21 (2006).
- De Gottardi, A. et al. Risk of complications after abdominal paracentesis in cirrhotic patients: a prospective study. Clin Gastroenterol Hepatol 7, 906-9 (2009).
- Wong, C.L., Holroyd-Leduc, J., Thorpe, K.E. & Straus, S.E. Does this patient have bacterial peritonitis or portal hypertension? How do I perform a paracentesis and analyze the results? JAMA 299, 1166-78 (2008).
- Barsuk, Jeffrey H., et al. “Vascular Ultrasonography: A Novel Method to Reduce Paracentesis Related Major Bleeding.” Journal of hospital medicine (2017): E1-E3.
